
Self Care for
Indian women
Indian women carry a continuous load across chores, child care, and elder care. The study tracks when self-care can happen, what hinders it, and how it fits into daily routines.
My Role
Qualitative Fieldwork
Video Lead
Literature Review
Team [6 members]





S
Timeline
4-5 Weeks (Jan 2025)
India
ranks
135 out of 146
countries in the
Global Gender Gap Ranking.


only
33%
of Indian women
have ever accessed the Internet.
just
51%
of Indian women
get to decide their Family Planning use.
Women: India & the World
Married women worldwide face discrimination, often being expected to prioritise domestic duties. This is amplified for Indian women due to:

Restricted movement and unsafe travel options that limit their independence, particularly at night.
Traditional family structures where they have minimal power and freedom, especially in joint families.
Cultural and workplace stigma that repeatedly discourages mothers from pursuing employment or careers.
Causal Map: detailing the lives of women in India

Family first, mother last
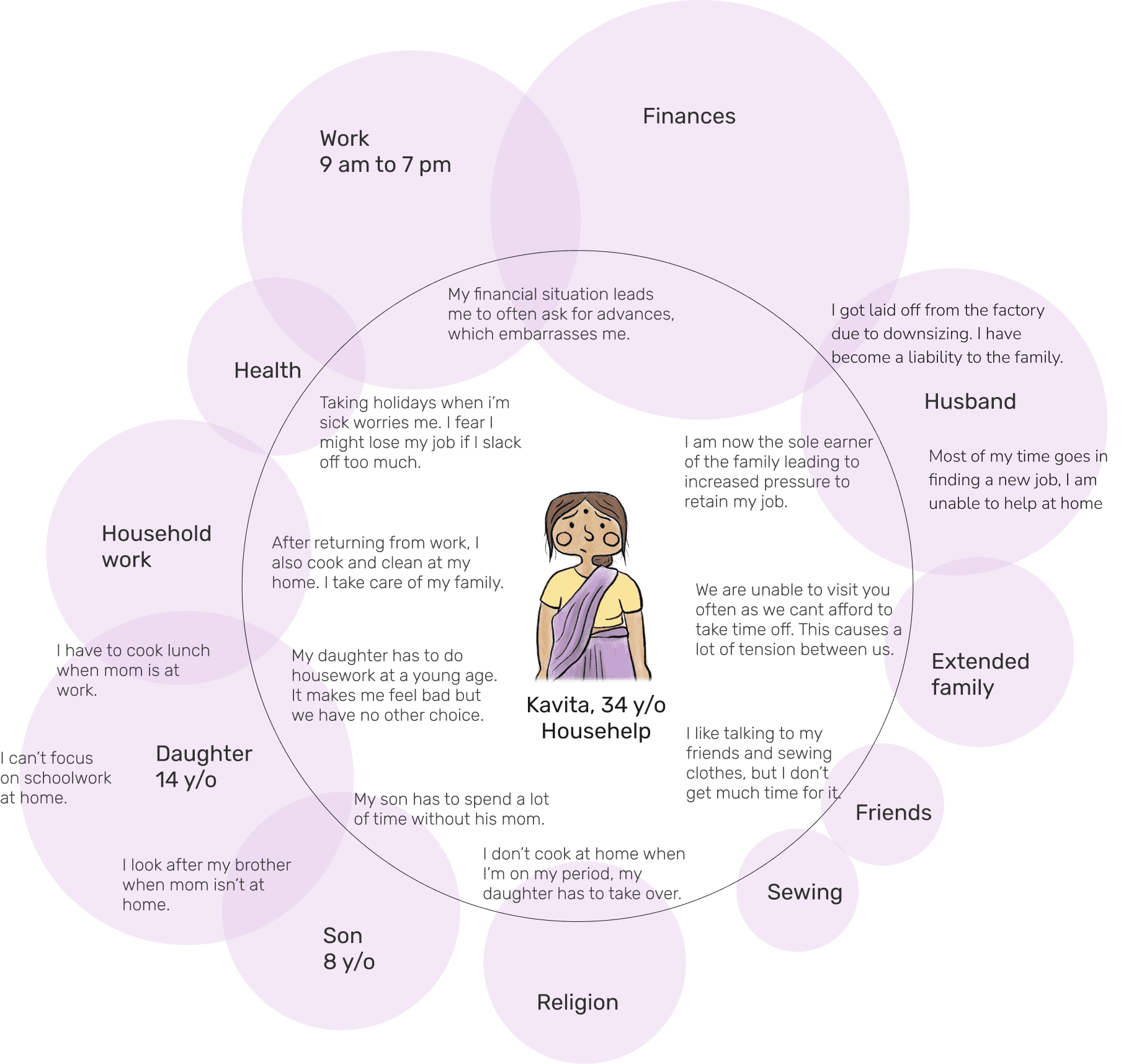
Cultural Model: Each bubble in this model is a ‘culture’ that influences her life. Bigger circles and greater overlaps indicate a stronger influence on Kavita’s life.
Illustrated below is the life of one of the women we interviewed (name changed), who is a housemaid in 2 of the houses in IIT Bombay. Her mind revolves around managing the family’s well-being and finances, leaving her own health largely neglected. She has very little time for the hobbies she enjoys, like sewing, or for bonding with friends.
With minimal support from her husband in caring for the children, she is forced to shoulder most responsibilities alone. Sadly, we can see her daughter being pulled into the same cycle of housework and family obligations, hindering her education and aspirations.
Despite exhaustion, Kavita holds the family together. Her story reflects the silent endurance of countless women balancing survival and duty.
Neglected Health
Merely
10%
of Indian women
reportedly allowed to take their own Healthcare decisions.

only
32%
of Indian women
had any contact with a healthcare worker.
53.2%
of non-pregnant Indian women are reported Anemic.
Contextual Inquiry
Research Method


The first problem for design is to understand the customers: their needs, their desires, their approach to the work. A customer-centered process makes an explicit step of understanding who the customers really are and how they work on a day-to-day basis.
Contextual design starts with one-on-one interviews with customers in their workplace while they work. These are followed by team interpretation sessions in which everyone can bring their unique perspective to bear on the data.
We visited women in Powai and Dahisar to speak with and observe their everyday lives in person. Through these conversations, we learned that they dedicate very little to no time of their days to self-care.
Their diets did not align with their health requirements, and they did not get enough exercise. Older women often dismiss their bodies’ signs of ageing and continue to work as they did when they were young.
Interview Excerpts
“I planned to open a food stall but my son is in 10th class (high school) and I have to look after his studies.”
“Real self-care for us is distancing and disconnecting from our husbands during fights.”
“Just a housewife”
Closer look at the Image of a woman in a
Traditional Indian Joint-Family Household

Extended family systems such as India’s, where family members of different generations co-reside, tend to allow for significant mobility within the household hierarchy. For an Indian woman this often means that her status in the household will increase as she passes key milestones.
A new bride enters her husband’s home as the lowest-status woman in the hierarchy, which increases as she becomes a mother and eventually a mother-in-law. She is made to leave school in her adolescence and is married to a man chosen by her parents.
She moves in with her husband’s family in the city, living among strangers and sacrificing her needs for theirs. Isolation, under-appreciation and her responsibilities as a wife and mother of two leave her burnt out by middle-age.
After marrying off her children, she finally gains autonomy and respect as a mother-in-law. However, by the time she is free of her burdens, she feels her life has already passed her by.
This is the story of Chandni
and it reflects the experiences of countless housewives in India.
The health of the Indian woman, both mental and physical, is inherently linked to her status in her family and in society.
465
million+
Indian Women are engaged in Unpaid household chores and caregiving.
Mapping Opportunities
Using a Priority Matirx
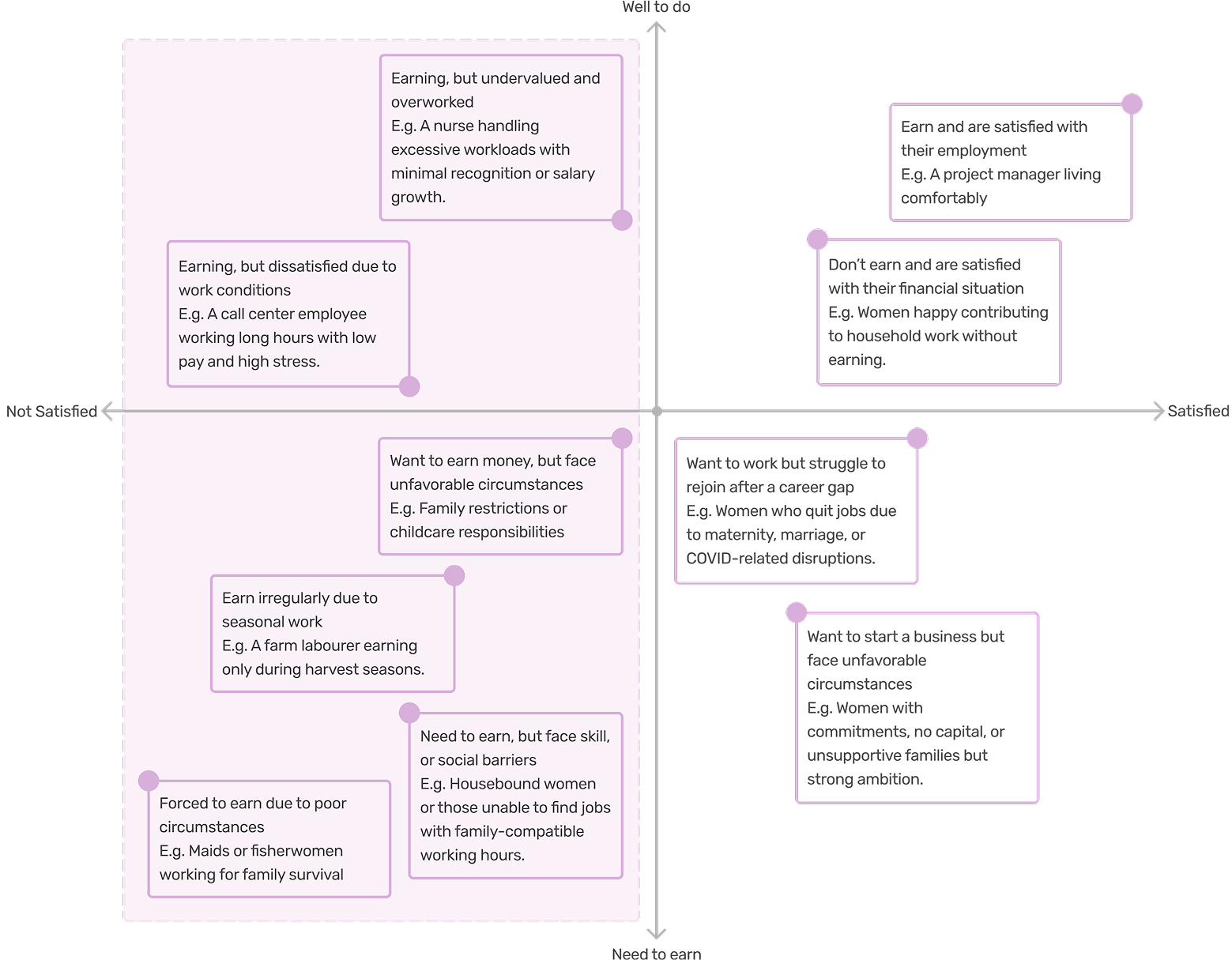
Priority Matrix: Mapping different situations an Indian woman can face across satisfaction and financial need axes, and choosing an area to focus on.

We have decided to focus on women who are either employed or unemployed and are unsatisfied with their situation. This can include both those who are too poor to quit and those whose aspirations are overlooked because there is “no need”.
Why is this important?
We believe that empowering women to balance taking care of their own selves along with taking care of their families can have a profound ripple effect that uplifts families and communities. The health of the woman is direct indicator of the health of a nation. Enabling women to choose for themselves will help unlock a vast reserve of human potential that lies latent.
Converged Problem Definition
How might we empower Indian women, who bear the bulk of household responsibilities, to inculcate self-care, social connection, and personal growth into their daily lives, without compromising their core priorities or loved ones’ needs?
i
Naman Khurana
© 2025. All rights reserved.